Collagen & Elastin
Collagen and elastin are the main structural proteins of the skin. Over time we lose collagen and elastin. This results in thinner and dryer skin which is more likely to wrinkle and sag. With repeated contraction of facial muscles, the thin, dry skin creates wrinkling over time. The “dynamic lines” which are wrinkles that only exist when engaging a facial muscle contraction eventually turn into “static lines” which are wrinkles present even while the face is at rest.
Clinical Pearl:
A collagen stimulator such as Sculptra, is a type of exogenous collagen therapy. When injected into the skin and subcutaneous tissue it triggers your body to produce new collagen.1 Collagen provides structural support for hyaluronic acid and elastin. Hyaluronic acid (HA) is a naturally occurring substance which acts as a lubricant and cushion. Hyaluronic acid attracts water molecules to restore skin moisture, while elastin provides elasticity and helps the skin stretch.
Another type of collagen induction therapy is microneedling with platelet rich plasma (PRP). The action of microneedling stimulates your body’s endogenous collagen production via tiny needles that make microscopic punctures in the skin. We can take this a step further by also using your own plasma, which is rich in growth factors, to gain additional improvement in the appearance of the skin. Patients notice improvements in skin tone, reductions in pore size, reductions in fine lines, improvements in acne scars, and improvements in stretch marks.
Fat Pads
Beneath our skin we have two compartments of fat pads in our face: one deep layer and one superficial layer. These fat pads support our skin and soft tissue. When we lose volume in these fat pads the result is a more sunken and hollow appearance.2 Descent of fat pads leads to the formation of jowls, smile lines, and hollow cheeks. Facial ligaments are important to help support and suspend the deep and superficial fat pads. With time these ligaments become stretched and lax, allowing further descent of the tissue.3
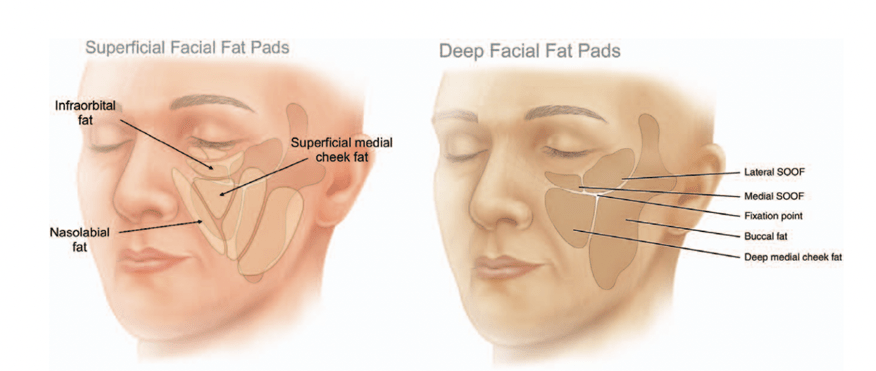
In a youthful face we always see full cheeks and defined cheekbones. While bony support from the zygoma contributes to this appearance, much of the cheek projection depends on the volume of the deep and superficial medial cheek fat pads. The zygomatic cutaneous ligament provides support of these fat pads helping to keep the tissue lifted. 3 This appearance can be called “the triangle of youth”. With age, the triangle inverts, and fullness falls to the lower face. This is caused by descent of the fat pads, adipose atrophy, and laxity of ligaments.
So how do we go about turning that triangle back around?
When we think about restoring facial fat atrophy and ligament laxity we must start from the top and work our way down.4 The tissue descent and laxity start in the upper and mid face. We want to address the root cause, not just the translations we are perceiving.
For example, if the lower face is the area of concern, we should first address the upper and mid face. We must restore the temples, cheeks, and piriform aperture before filling the nasolabial folds or the pre-jowl sulcus. If we merely fill the lines, we see we are not addressing the origin of the problem and often patients are left with an unnatural appearance.

Bones
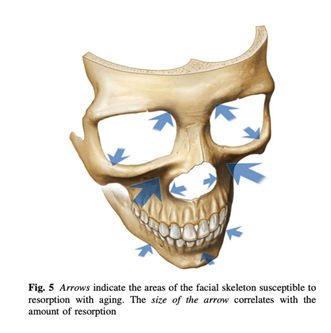
Over time the process of aging results in gradual bone loss that contributes to changes in the structure of our faces. Faces become longer, wider, and deeper due to bone resorption.5 When bone resorption occurs this also alters the attachment of facial support ligaments, muscles, and fat pads.
In the periorbital region the orbital aperture increases in width and height. This is most noticeable in the lower outer orbital rim and the upper inner orbital rim.5
The bony anatomy of the midface consists of the maxilla and zygoma. There is evidence that both bones are subject to retrusion. Maxillary retrusion is more common, more noticeable, and occurs at younger ages. Widening of the nasal bones and retrusion of the piriform aperture leads to change in the shape and position of the nose as well as contributes to deep nasolabial folds, also known as “smile lines”.
Retrusion in the lower face (mandible) results in a reduction in the projection of the chin and increased “jowling” of the soft tissue.
Clinical Pearl:
Rebuilding the skeletal support with fillers helps improve projection and assists in repositioning the soft tissue. It’s essential to start “from the ground up” when we look to restore volume loss. With age, the maxilla retrudes and the nasal bones widen, so injecting a dense filler with high lifting capability to the piriform aperture is imperative for a patient complaining of deep nasolabial folds. Injecting superficially into the skin is not correcting the root cause of the problem which is bone loss and retrusion. We need to start with deep restoration as this will change the position of the overlying skin soft tissue, ligaments, and fat pads.